 CBP®, also known as Chiropractic BioPhysics® or Clinical Biomechanics of Posture® is a particular type of Chiropractic care that helps produce optimal posture and spinal alignment. As your spine assumes a more ideal shape and relationship with gravity, symptoms often diminish and health may often return. This diagnostic and treatment protocol is one of if not the most researched and published approaches to spinal health in Chiropractic or manual therapy.
CBP®, also known as Chiropractic BioPhysics® or Clinical Biomechanics of Posture® is a particular type of Chiropractic care that helps produce optimal posture and spinal alignment. As your spine assumes a more ideal shape and relationship with gravity, symptoms often diminish and health may often return. This diagnostic and treatment protocol is one of if not the most researched and published approaches to spinal health in Chiropractic or manual therapy.
What is CBP®
In December 1980, Chiropractic BioPhysics® or CBP® Technique was originally named by Drs. Donald Harrison, Deanne Harrison, and Daniel Murphy for “physics applied to biology in chiropractic”.
Since that time, Drs. Donald and Deed Harrison, (along with a number of other contributors) have authored Seven CBP® Texts Books and published more than 130 scientific studies investigating different aspects of CBP®.1-7
Thus, today, CBP® Technique is one of if not the most investigated techniques in Chiropractic and both Drs Harrison are among the leaders in the profession’s researchers.
CBP® Goals of Care
CBP® Technique emphasises optimal posture and spinal alignment as the primary goals of chiropractic care while simultaneously documenting improvements in pain and functional based outcomes (See Figure 1). The uniqueness of CBP® treatment is in the structural rehabilitation of the spine and posture. In general, the goals of CBP® Care are:
1. Normal Front & Side View Posture
1. Center of mass of head, rib cage & pelvis vertically aligned in Front and Side views.
2. Normal Spinal Alignment
a. Front view: vertical alignment
b. Side View: Harrison Ideal or Average Spinal Model
3. Normal function
a. Improved Range of Motion and quality of movement,
b. Improved muscle strength,
1. Improved Health & Symptom Improvements
1. Neck disability index
2. Oswestry low back index,
3. SF 36 or Health Status Questionaire
Ideal Postural Alignment:
 CBP® Chiropractic BioPhysics®
CBP® Chiropractic BioPhysics®
Figure 1. Ideal postural alignment is depicted in both the frontal and side views. In each view, the centre of mass of the skull, thorax, and pelvis are in a vertical line with respect to gravity. In the frontal view, the spinal column is vertically aligned a straight column with respect to gravity. In the side view, the spine has three primary curvatures which will be described below:
1. Neck Curve - Cervical Lordosis, 2. Ribcage Curve - Thoracic Kyphosis, 3. Low back Curve - Lumbar Lordosis
Ideal Spinal Alignment with CBP®: Harrison Full Spine Model
As in all fields of study dealing with the human body, there exist normal values for alignment of the spine. The Harrison Spinal Model is an evidenced-based model for side view spinal alignment. It is the geometric path of the posterior longitudinal ligament or the backs of the vertebra from the 1st neck vertebra to the bottom of the lower back or top of the sacrum. See Figures 3-6 below detailing the Harrison Spinal Model.
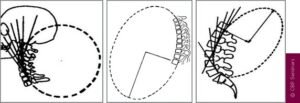
CBP® researchers have extensively published ideal and average models for the human spinal curvatures as viewed from the side. This research has lead to the finding of the ‘Harrison Spinal Model’. This model details both Ideal and Average geometric shapes for the curves of the spine from the side. Additionally, ideal and average ranges for the spinal segmental angles for each of the spinal regions have been identified. The model suggests the neck or cervical spine should have a geometric shape that approximates a ‘piece of a circle’. The ribcage or thoracic spine should have a geometric shape that approximates an oval-elliptical shape. And the low back or lumbar spine should have a geometric shape that approximates an oval-elliptical shape.26-31
These are “evidence-based” models. In fact, the CBP® neck-cervical circular model27 and the low back- lumbar elliptical model29 have both been found to have discriminative validity between pain and non-pain subjects. In other words, the Harrison Spinal Model has been found to be able to identify pain subjects versus non-pain subjects by what their spinal x-ray shapes are.
 CBP® Chiropractic BioPhysics®
CBP® Chiropractic BioPhysics®
Figure 3. The three figures above demonstrate the concept that each spinal region has a normal geometry or shape of the spinal curves. On the readers left is the neck or cervical spine. Here the shape of the neck curve should approximate a piece of a circle. In the centre is the ribcage or thoracic spine. Here the shape in the ribcage should approximate a piece of an oval or ellipse. On the right is the lower back or lumbar spine. Here the shape in the lower back should approximate a piece of an oval or ellipse.
 CBP® Chiropractic BioPhysics®
CBP® Chiropractic BioPhysics®
Figure 4. The Harrison Full Spine Model (above). On the readers left is the exact geometric model of the side view of the spinal curves as identified by Harrison and colleagues. This model can be used to evaluate a given patient’s side view of the spine. For example, a full spine x-ray on the right is shown. The red curved line represents the Harrison spinal model, and this shows where the model predicts the patient’s spine should be lined up. It is apparent that this patient has altered spinal alignment as they do not fit even close to the Harrison Idealized Spinal Model.
 CBP® Chiropractic BioPhysics®
CBP® Chiropractic BioPhysics®
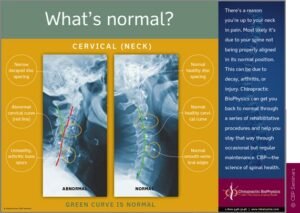
Figure 5. The Harrison Spinal Model in the Neck-Cervical region. The Harrison spinal model is depicted as the GREEN curved line in this figure. On the Right is a normal curved patient x-ray. On the left is an abnormal curved patient x-ray; where the patient’s neck shape is shown by the red dashed line. The Harrison Spinal Model in the neck has been shown to reasonably predict which person will have neck pain compared to normal subjects.
The Harrison Spinal Model in the low back has been shown to reasonably predict which person will have low back pain compared with normal subjects.
CBP® Mirror Image® Spinal Traction
The originators and developers of CBP used specific exercises and adjustments in the “Mirror Image” to effect change in spine shape and posture. In difficult cases they also added and developed “Mirror Image” postural and spinal traction.
Postural mirror image and extension traction for the side view spinal curves provides sustained loading periods of 10-20 minutes and is necessary to cause visco-elastic deformation to the resting length of the spinal ligaments, muscles, and discs.52
There are MANY types of spinal extension traction methods used in CBP® Technique; some are more aggressive and technical than others. Whereas some forms of spinal extension traction are available for patients to use at home; the examples shown in Figures 13-14 are in office types only. Note: Each patients spine is unique and thus, a variety of traction devices are used depending upon the exact condition of the patient.
 CBP® Chiropractic BioPhysics®
CBP® Chiropractic BioPhysics®
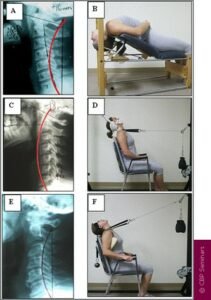
Figure 13. Three different spine shapes (abnormal alignment) of the cervical curve and their respective Mirror Image traction methods. In A, hypolordosis with mild anterior head translation requires compression extension traction in B. In C, slight kyphosis with posterior head translation requires 2-way non-compression traction in D. In E, reversal of the upper cervical curve with mild anterior head translation requires compression extension 2-way traction in F.4,14-16
 CBP® Chiropractic BioPhysics®
CBP® Chiropractic BioPhysics®
Figure 14. Two different examples of an aberrant lumbar curve and one of the thoracic curve and their respective Mirror Image traction methods. In A, lumbar kyphosis with anterior thoracic translation requires 3-point bending extension traction in B (shown standing). In C, slight lumbar kyphosis with posterior thoracic translation requires 3-point bending in D (shown supine). In E, hyper-kyphosis of the thoracic curve requires 3-point bending thoracic traction in F (shown standing).
CBP®Treatment Interventions
The CBP® protocol of care recommends that relief care (traditional chiropractic management) be separated from structural rehabilitation of the spine and posture. In this regard, the typical patient would receive an initial short period of care aimed at improving segmental and overall spinal range of motion (RoM) and pain intensity/frequency. Treatment interventions/methods would consist of any number of segmental adjusting techniques the chiropractor prefers to utilise (Diversified, Gonstead, Activator, etc ).
After, the initial relief care examination, for those who choose CBP® structural rehabilitation procedures would begin and include Mirror Image® exercises, adjustments, and traction (referred to as the E.A.T protocol). The use of a combination of postural mirror image exercises, adjustments, and traction procedures attempts to address as much as possible in the tissues and mechanisms involved in spine and posture alignment.
References-
1 Harrison DD. CBP Technique: The Physics of Spinal Correction. National Library of Medicine #WE 725 4318C, 1982-97. Harrison DD. CBP Technique: The Physiscs of Spinal Correction. 2 Harrison DD. Spinal Biomechanics: A Chiropractic Perspective. National Library of Medicine #WE 725 4318C, 1982-97. Harrison DD. CBP Technique: The Physiscs of Spinal Correction. 3 Harrison DD. CBP X-ray Work Book. National Library of Medicine #WE 725 4318C, 1982-97. Harrison DD. CBP Technique: The Physiscs of Spinal Correction. 4 Harrison DE, Harrison, DD, Haas JW. CBP® Structural Rehabilitation of the Cervical Spine. Evanston, WY: Harrison CBP Seminars, 2002. 5 Harrison DE, Harrison, DD, Haas JW, Oakley PA. Spinal Biomechanics for Clinicians, Volume I. Evanston, WY: Harrison CBP Seminars, 2003. 6 Harrison DE, Harrison, DD, Haas JW, Oakley PA. CBP® Structural Rehabilitation of the Lumbar Spine. Evanston, WY: Harrison CBP Seminars, 2005. 7 Harrison DE, Betz J, Harrison, DD. CBP® Structural Rehabilitation of the Thoracic Spine. Evanston, WY: Harrison CBP Seminars, 2005. 8 Chiropractic Biophysics Online. http://www.idealspine.com/. Services/research papers. Accessed 12-15-04. 9 Harrison DD, Janik TJ, Harrison GR, Troyanovich SJ, Harrison DE, Harrison SO. Chiropractic Biophysics Technique: A Linear Algebra Approach to Posture in Chiropractic. J Manipulative Physiol Ther 1996;19(8):525-535. 10 Panjabi MM, White AA, Brand RA. A Note on Defining Body Parts Configurations. J Biomech 1974; 7:385. 11 Harrison DE, Harrson DD. The Lumbar Spine: Rehabilitation with the CBPâ method. National Library of Medicine #WE 725 4318C, 1997. 12 Harrison DE, et al. Changes in sagittal lumbar configuration with a new method of extension traction. Presented at the 27th annual meeting of the International Society for the Study of the Lumbar spine. Adelaide, Australia April 9-13, 2000;151. 13 Harrison DE, Harrison DD, Cailliet R, Janik TJ, Holland B. Changes in Sagittal Lumbar Configuration with a New Method of Extension Traction: Non-randomized Clinical Control Trial. Arch Phys Med Rehab 2002;83(11):1585-1591. 14 Harrison DD, Jackson BL, Troyanovich SJ, Robertson GA, DeGeorge D, Barker WF. The Efficacy of Cervical Extension-Compression Traction Combined with Diversified Manipulation and Drop Table Adjustments in the Rehabilitation of Cervical Lordosis. J Manipulative Physiol Ther 1994;17(7):454-464. 15 Harrison DE, Harrison DD, Betz J, Colloca CJ, Janik TJ, Holland B. Increasing the Cervical Lordosis with Seated Combined Extension-Compression and Transverse Load Cervical Traction with Cervical Manipulation: Non-randomized Clinical Control Trial. J Manipulative Physiol Ther 2003; 26(3): 139-151. 16 Harrison DE, Cailliet R, Harrison DD, Janik TJ, Holland B. New 3-Point Bending Traction Method of Restoring Cervical Lordosis Combined with Cervical Manipulation: Non-randomized Clinical Control Trial. Arch Phys Med Rehab 2002; 83(4): 447-453. 17 Harrison DE, Cailliet R, Betz JW, Harrison DD, Haas JW, Janik TJ, Holland B. Harrison Mirror Image Methods for Correcting Trunk List: A Non-randomized Clinical Control Trial. Eur Spine J 2004; In Press. 18 Harrison DE, Harrison DD, Haas JW, Betz JW, Janik TJ, Holland B. Conservative Methods to Correct Lateral Translations of the Head: A Non-randomized Clinical Control Trial. J Rehab Res Devel 2004;41(4):631-640. 19 Zaleski BW, Wood J. A comparison of Palmer package and Chiropractic Biophysics for the treatment of pain. Proceedings of the International Conference on Spinal Manipulation 1992; Chicago, IL., May 15-17. 20 Paulk GP, Bennett DL, Harrison DE. Management of a chronic lumbar disk herniation with CBP methods following failed chiropractic manipulative intervention. J Manipulative Physiol Ther 2005;in press. 21 Ferrantelli JR, Harrison DE, Harrison DD, Steward D. Conservative management of previously unresponsive whiplash associated disorders with CBP methods: a case report. J Manipulative Physiol Ther 2005;in press. 22 Haas JW, Harrison DE, Harrison DD, Bymers B. Reduction of symptoms in a patient with syringomyelia, cluster headaches, and cervical kyphosis. J Manipulative Physiol Ther 2005;in press. 23 Harrison DE, Bula J. Non-operative correction of the flexible flat back using lumbar extension traction: A case study of three. J Chiropractic Education 2002;16(1). 24 Bastecki A, Harrison DE, Haas JW. ADHD: A CBP case study. J Manipulative Physiol Ther 2004; 27(8):e14. 25 Harrison DE, Harrison DD. Chiropractic Biophysics Technique. Part I: The Scientific Basis. Eur Chiropractic J 2005; 26 Harrison DD, Janik TJ, Troyanovich SJ, Holland B. Comparisons of Lordotic Cervical Spine Curvatures to a Theoretical Ideal Model of the Static Sagittal Cervical Spine. Spine 1996;21(6):667-675. 27 Harrison DD, Harrison DE, Janik TJ, Cailliet R, Haas JW, Ferrantelli J, Holland B. Modeling of the Sagittal Cervical Spine as a Method to Discriminate Hypo-Lordosis: Results of Elliptical and Circular Modeling in 72 Asymptomatic Subjects, 52 Acute Neck Pain Subjects, and 70 Chronic Neck Pain Subjects. Spine 2004; 29:2485-2492. 28 Janik TJ, Harrison DD, Cailliet R, Troyanovich SJ, Harrison DE. Can the Sagittal Lumbar Curvature be Closely Approximated by an Ellipse? J Orthop Res 1998; 16(6):766-70. 29 Harrison DD, Cailliet R, Janik TJ, Troyanovich SJ, Harrison DE, Holland B. Elliptical Modeling of the Sagittal Lumbar Lordosis and Segmental Rotation Angles as a Method to Discriminate Between Normal and Low Back Pain Subjects. J Spinal Disord 1998; 11(5): 430-439. 30 Harrison DE, Janik TJ, Harrison DD, Cailliet R, Harmon S. Can the Thoracic Kyphosis be Modeled with a Simple Geometric Shape? The Results of Circular and Elliptical Modeling in 80 Asymptomatic Subjects. J Spinal Disord Tech 2002; 15(3): 213-220. 31 Harrison DD, Harrison DE, Janik TJ, Cailliet R, Haas JW. Do Alterations in Vertebral and Disc Dimensions Affect an Elliptical Model of the Thoracic Kyphosis? Spine 2003; 28(5):463-469. 32 Harrison DE, Harrison DD, Cailliet R, Troyanovich SJ, Janik TJ. Cobb Method or Harrison Posterior Tangent Method: Which is Better for Lateral Cervical Analysis? Spine 2000; 25: 2072-78. 33 Harrison DE, Cailliet R, Harrison DD, Janik TJ, Holland B. Centroid, Cobb or Harrison Posterior Tangents: Which to Choose for Analysis of Thoracic Kyphosis? Spine 2001; 26(11): E227-E234. 34 Harrison DE, Harrison DD, Janik TJ, Harrison SO, Holland B. Determination of Lumbar Lordosis: Cobb Method, Centroidal Method, TRALL or Harrison Posterior Tangents? Spine 2001; 26(11): E236-E242. 35 Harrison DE, Holland B, Harrison DD, Janik TJ. Further Reliability Analysis of the Harrison Radiographic Line Drawing Methods: Crossed ICCs for Lateral Posterior Tangents and AP Modified Risser-Ferguson. J Manipulative Physiol Ther 2002; 25: 93-98. 36 Harrison DE, Harrison DD, Colloca CJ, Betz J, Janik TJ, Holland B. Repeatability of Posture Overtime, X-ray Positioning, and X-ray Line Drawing: An Analysis of Six Control Groups. J Manipulative Physiol Ther 2003; 26(2): 87-98. 37 Haas M, Taylor JAM, Gillette RG. The routine use of radiographic spinal displacement analysis: a dissent. J Manipulative Physiol Ther 1999;22:254-259. 38 Phillips RB. Plain film radiography in chiropractic. J Manipulative Physiol Ther 1992;15:47-50. 39 Taylor JAM. Full-spine radiography: a review. J Manipulative Physiol Ther 1993;16:460-474. 40 Kauffman JM. Diagnostic radiation: are the risks exaggerated? J Amer Phys Surg 2003;8(2):54-55. 41 Cohen BL, Lee IS. A catalog of risks. Health Physics 1979;36:707-722. 42 International Atomic Energy Agency. Facts about low-level radiation. American Nuclear Society, 1982. 43 Janik TJ, Harrison DE, Cailliet R, Harrison DD, Normand MC, Black P. Validity of an algorithm to estimate 3-D rotations and translations of the head in upright posture from three 2-D digital images. 2005; In Review. 44 Harrison DE, Janik TJ, Cailliet R, Harrison DD, Normand MC, Black P, Perron DL. Validation of an algorithm to estimate 3-D rotations and translations of the thorax and pelvis in upright posture from three 2-D digital images. 2005 In Review. 45 Bolton JE. The evidence in evidence-based practice: what counts and what doesn’t count? J Manipulative Physiol Ther 2001;24:362-366. 46 Hrysomallis C, Goodman C. A review of resistance exercise and posture realignment. J Strength Cond Res 2001;15:385-390 47 Den Boer WA, Anderson PG, Limbek JV, Kooijman MAP. Treatment of idiopathic scoliosis with side shift therapy: An initial comparison with a brace treatment historical cohort. European Spine J 1999;8:406-410. 48 Weiss HR. Influence of an in-patient exercise program on scoliotic curve. Ital J Orthop Traumatol 1992; 18:395-406. 49 Weiss HR, Lohschmidt K, el-Obeidi N, Verres C. Preliminary results and worst-case analysis of in patient scoliosis rehabilitation. Pediatr Rehabil 1997;1:35-40. 50 Pearson ND, Walmsley RP. Trial into the effects of repeated neck retractions in normal subjects. Spine 1995; 20(11): 1245-51.). 51 DeVocht JW, Pickar JG, Wilder DG. EMG activity levels of paraspinal muscles during spinal manipulation. Proceedings from the 29th annual meeting of ISSLS 2002; Vancouver, Canada. 52 Oliver MJ, Twomey LT. Extension creep in the lumbar spine. Clin Biomech 1995;10:363-368. 53 Harrison DE, Harrison DD, Troyanovich SJ. Three-Dimensional Spinal Coupling Mechanics. Part II: Implications for Chiropractic Theories and Practice. J Manipulative Physiol Ther 1998; 21(3): 177-86. 54 Harrison DE, Cailliet R, Harrison DD, Troyanovich SJ, Janik TJ. Cervical Coupling on AP Radiographs During Lateral Translations of the Head Creates an S-Configuration. Clin Biomech 2000; 15(6): 436-440. 55 Harrison DE, Cailliet R, Harrison DD, Janik TJ, Troyanovich SJ, Coleman RR. Lumbar Coupling During Lateral Traction.
IdealSpine.com. 1998. What is CBP®. [ONLINE] Available at: http://idealspine.com/what-is-cbp/. [Accessed 24 July 2016].